
Gyne Blog
Uterine Fibroids
It is a benign tumor of variable size originating from the muscle cells that form part of the uterine or womb wall.
What is a fibroid?
It is a benign tumor of variable size originating from the muscle cells that form part of the uterine or womb wall.
It is also known as a fibroma, leiomyoma, or fibroleiomyoma.
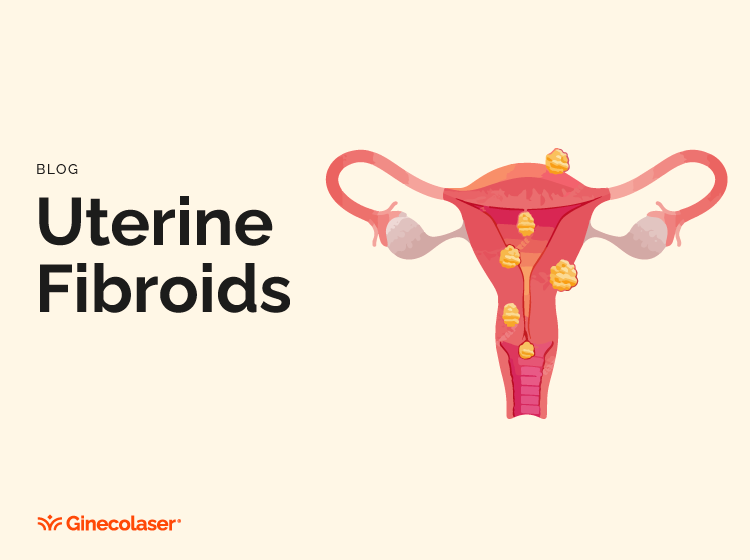
There are several types of fibroids according to their location:
- Submucosal: grow beneath the inner lining of the uterus towards its interior.
- Subserosal: grow beneath the outer layer of the uterus towards the exterior.
- Intramural: Grow within the muscular wall of the uterus.
- Pedunculated: have a stalk that connects them to the outer layer or the interior of the uterus.
- Depending on the location and size of the fibroid, the clinical manifestations will be different, ranging from producing no discomfort to causing significant symptoms
How are fibroids formed?
Uterine fibroids are very common tumors in women of reproductive age (from the first menstruation to menopause), being the leading cause of benign gynecological tumors.
Approximately 70% of women may have a fibroid, although most of them will not have symptoms. Their frequency increases with age, especially from thirty-five to forty onwards.
The cause of fibroids is unknown. However, it is known that their growth is influenced by female sex hormones, estrogen, and progestogens. Normally, their size increases during pregnancy and reproductive stages and decreases during menopause. Although uterine fibroids can be solitary, they are most commonly multiple and of varying sizes, ranging from small millimeters to several centimeters.
Are there any risk factors for having fibroids?
Several risk factors have been associated with an increased frequency of uterine fibroid occurrence, the most prominent ones being:
- Race, common in black women.
- Early onset of menstruation, having the first menstruation at an early age favors the appearance of fibroids.
- Number of children, women without children have a higher risk of developing fibroids.
- Age: higher prevalence in women over forty years old.
- Obesity, obese women have a higher risk of presenting fibroids due to higher levels of estrogen in the blood.
- Family history, some fibroids seem to have a genetic component and are more common among first-degree relatives (mothers and sisters).
- Sedentary lifestyle, it has been observed that exercise significantly decreases the risk of developing fibroids.
How do I know if I have a fibroid?
Many fibroids do not produce symptoms, are asymptomatic, and are an incidental finding during gynecological examination.
Those that do produce symptoms will present:
- Bleeding abnormalities, irregular, prolonged bleeding between menstruations, and excessive bleeding.
- Pelvic discomfort or lower abdominal pain.
- Discomfort during sexual intercourse.
- Symptoms of pressure on the bladder, difficulty urinating, or frequent urination.
- Symptoms of compression on the rectum, leading to constipation and irritability.
How are fibroids diagnosed?
Generally, fibroids are diagnosed through a proper medical history and gynecological examination. In addition to medical history and examination, complementary studies, mainly imaging studies, can be performed, such as:
- Transvaginal ultrasound is one of the most useful methods for diagnosing fibroids, allowing the location and size of the fibroids to be determined.
- Hysterosonography is an ultrasound technique in which the uterus is filled with saline solution to distend it and thus better visualize its interior.
- Hysteroscopy is a visual examination of the inside of the uterus performed by inserting a camera through the vagina. It is very useful for assessing the size and location of fibroids and their resection.
- Hysterosalpingography, a radiological examination that allows visualization of the uterus using contrast.
- Magnetic resonance imaging is the most accurate imaging test and is usually used to thoroughly study fibroids before surgery.
How are fibroids treated?
The treatment of fibroids depends on multiple factors such as the woman's age, whether she has children, whether she wants to have children in the future, the type and size of fibroid, the severity of symptoms, and the woman's overall health.
The vast majority require periodic examination as part of routine checks because they usually do not cause symptoms, and there are currently various options that allow treatment to be individualized based on the patient's characteristics.
Among surgical treatments, there may be different types considering some of the symptoms and to remove the fibroids, myomectomy, the removal of fibroids while preserving the uterus, is usually done abdominally, vaginally laparoscopically, and in those women who wish to have children.
Hysterectomy is a more radical treatment where the uterus is removed and is usually done abdominally, vaginally laparoscopically, and is used when other treatments fail or when the woman does not wish to have more children.
FAQs
Can fibroids recur after treatment except in the case of surgical treatment through hysterectomy, in which the uterus is completely removed, and therefore any possibility of a fibroid reappearing in the rest of the treatments may occur.
Can fibroids become cancerous?
Fibroids are benign tumors and very rarely become malignant, less than 1%, and it is believed that these cancers do not originate from the existing fibroid but from an associated pathology.